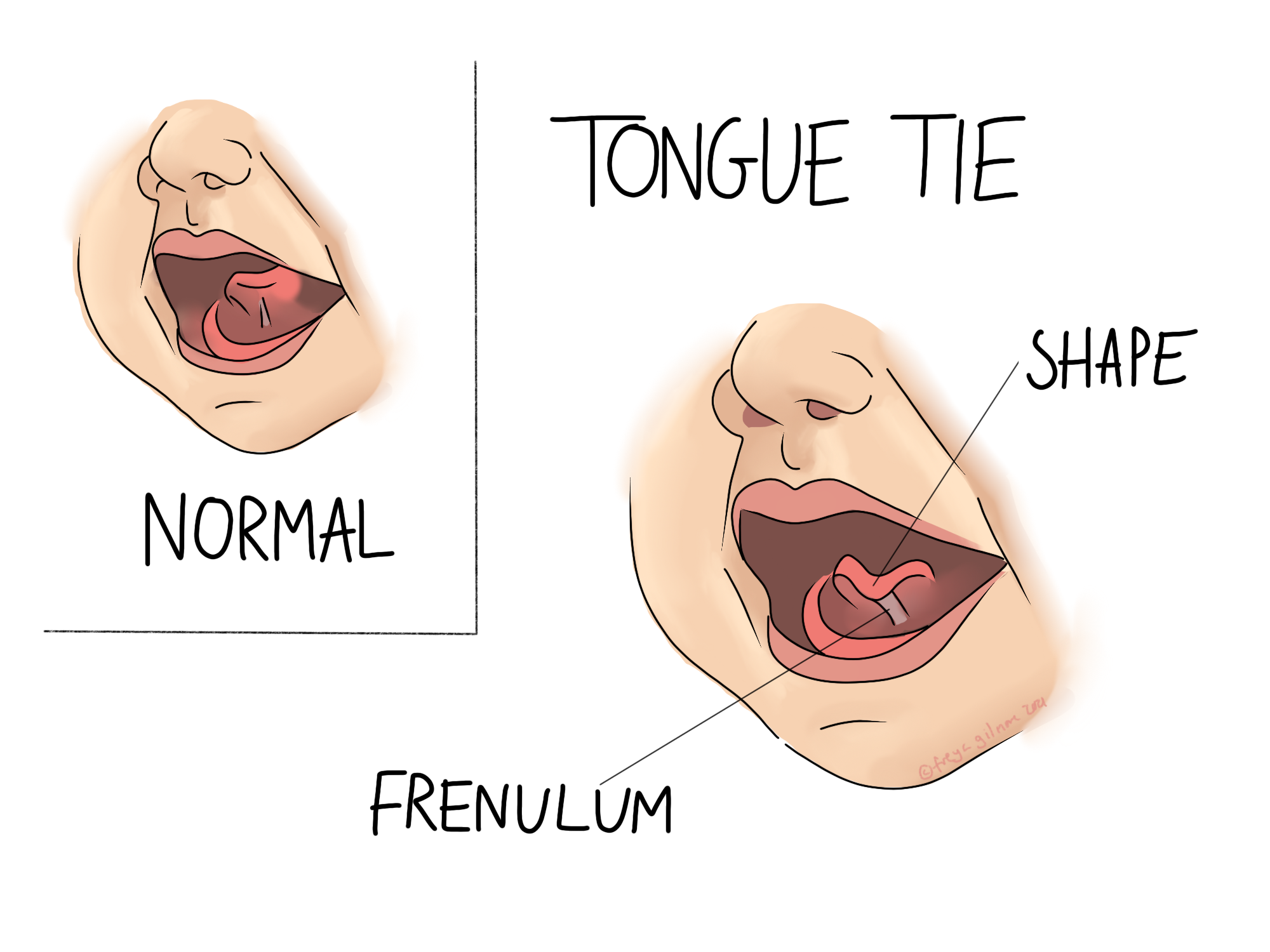
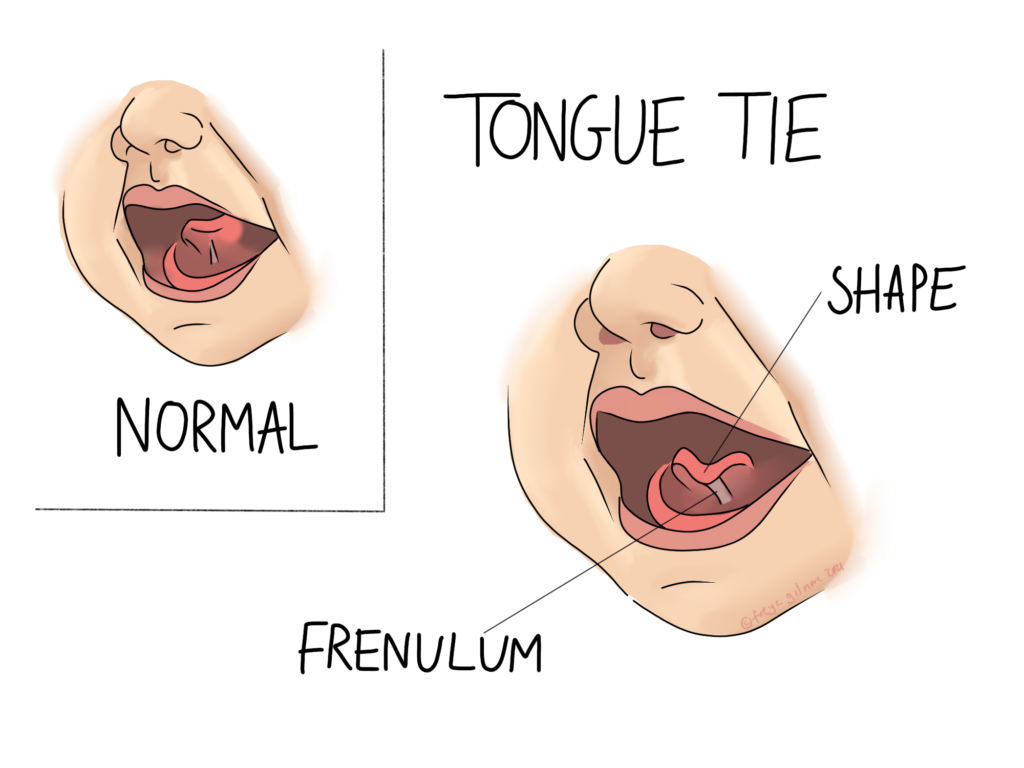
Some babies are born with reduced mobility in their tongue. This can make feeding inefficient, and painful for the mother if breastfeeding. The cause may be a tongue tie- a short or thick frenulum, which is the tissue that connects the tongue to the base of the mouth.
Diagnosing Tongue Tie
Diagnosis takes a skilled practitioner and in the first instance if experiencing feeding issues you should make contact with your Infant Feeding Team. It is much more important how the tongue moves than what it looks like- we all have a frenulum so seeing tissue under the tongue may well be normal.
If the frenulum is very restrictive, especially at the front of the tongue, movement may be visibly diminished when crying. We expect the tongue to raise when the baby cries with an open mouth. More severe cases will come with a “heart shaped” tongue on this movement. The centre of the tongue cannot lift, so only the sides raise as normal, and a valley is left in the centre.
In addition to nipple pain tongue tie might present with
- Failure to clear milk from the tongue. This leaves a white layer that may be mistaken for thrush
- Noisy feeding at breast or bottle
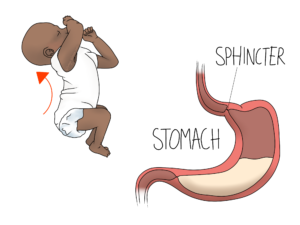
- Taking on a lot of air at feeds, gassiness
- Short and frequent feeding
These symptoms are signs of a shallow latch, but not all latch issues are due to tongue tie. Thorough feeding assessment is required to determine the cause the best route forward.
Treatment Options
If a tongue tie is sufficiently restricting tongue function you will be offered a frenotomy- a surgical procedure involving, most commonly a scissor cut the the tight frenulum.
An Osteopath may be involved before and/or after to help with the mechanical element of restriction. Although the frenulum is not a muscle, and cannot be stretched we can work on the muscles and connective tissues around the tongue, jaw and face to help ease associated tensions.
This involves direct work within your baby’s mouth, with gloved fingers. Before any treatment is carried out, your osteopath will explain what they want to do and gain consent from you. This conversation will include risks and benefits. To maintain the benefit, you may be asked to continue similar exercises at home between treatments. We often work with other professionals- latch issues are best supported by a qualified feeding expert (such as your NHS Infant Feeding Team or a private lactation consultant)
The Bigger Picture
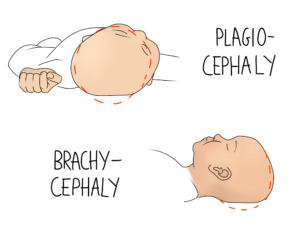
If your baby has been struggling to latch they may develop their own way of feeding that creates different tensions in the body. Your osteopath will look for compensatory patterns and work to resolve them. Common problematic areas include the diaphragm and shoulders, or the neck. If the neck is involved, there may be susceptibility to favouring turning head to one side and developing plagiocephaly (or “flat head syndrome”). Your osteopath can tie all of these factors together to develop a personalised treatment plan for your baby.